GFR Calculator:
Estimate Your eGFR
& Kidney Function Free
Your eGFR (estimated Glomerular Filtration Rate) is the most important single number for understanding how well your kidneys are functioning. This free GFR calculator uses the gold-standard CKD-EPI 2021 equation — along with MDRD and Cockcroft-Gault for reference — to estimate your kidney function from your serum creatinine blood test result, age, and biological sex.
A normal eGFR for adults is 90 mL/min/1.73m² or above. An eGFR below 60 sustained for three or more months indicates Chronic Kidney Disease (CKD). GFR naturally declines approximately 1 mL/min/1.73m² per year after age 40, so age context is important when interpreting your result.
⚠️ This eGFR calculator is for educational use only. It does not replace laboratory measurement or clinical interpretation by a qualified healthcare professional. If your result is below 60, please consult your doctor promptly.
eGFR / Kidney Function Calculator
NKF-Endorsed 2021Enter value in mg/dL. Normal adult range: 0.6–1.2 mg/dL (males), 0.5–1.1 mg/dL (females).
| Formula | eGFR Result | Best Used For |
|---|---|---|
| CKD-EPI 2021 | — | CKD diagnosis & staging (recommended) |
| MDRD 4-var | — | Reference / established CKD patients |
What Is GFR? Understanding Your Glomerular Filtration Rate
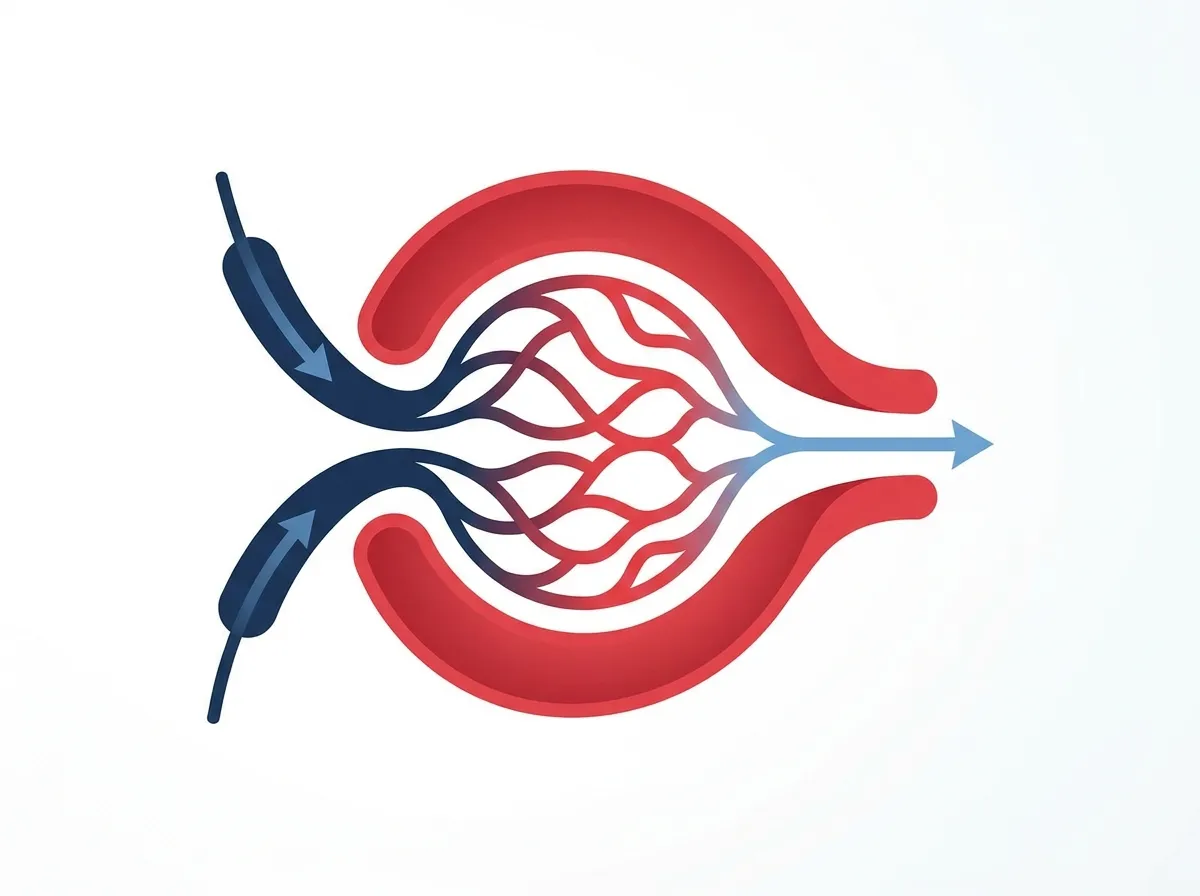
The Glomerular Filtration Rate (GFR) is the volume of fluid filtered from your blood through the tiny capillary networks inside your kidneys — called glomeruli — every minute. It is the single most reliable indicator of overall kidney function available in routine clinical practice, and it is the measurement that determines whether you have Chronic Kidney Disease (CKD) and, if so, which stage.
Each of your kidneys contains approximately one million microscopic filtering units called nephrons. Each nephron contains a glomerulus — a tiny knot of capillaries that filters waste products, excess fluid, and toxins out of your blood while keeping essential proteins, cells, and nutrients in the bloodstream. GFR measures the combined efficiency of all these filters working simultaneously.
Because directly measuring GFR requires complex, invasive testing using external filtration markers like inulin — impractical for everyday clinical use — physicians rely on the estimated GFR (eGFR), calculated from a blood test measuring serum creatinine alongside your age and biological sex. The Heart Score Calculator's GFR calculator uses the CKD-EPI 2021 equation, which is currently the most accurate and equitable formula recommended by both the National Kidney Foundation and the American Society of Nephrology.
Understanding your eGFR is particularly important because an estimated 37 million adults in the United States may have chronic kidney disease, but nearly 90% are unaware of their condition. Early detection through regular eGFR testing — especially if you have diabetes, high blood pressure, or a family history of kidney disease — can prevent progression to more severe stages where dialysis or transplantation becomes necessary.
Kidney health is closely intertwined with cardiovascular health — a connection that the Heart Score Calculator was specifically designed to help people understand. Reduced kidney function is an independent risk factor for heart attack, stroke, and all-cause mortality, which is why monitoring both your eGFR and your cardiovascular risk profile together gives you a far more complete picture of your overall health.
Normal GFR Range by Age: What to Expect at Every Decade
A healthy adult under 40 typically has an eGFR between 100 and 130 mL/min/1.73m². However, GFR naturally declines with age at approximately 0.7 to 1.0 mL/min/1.73m² per year after age 40 — even in people with perfectly healthy kidneys. This age-related decline reflects the gradual reduction in the number of functioning nephrons, decreased renal blood flow, and changes in glomerular structure that are a normal part of the aging process.
This is why an eGFR of 72 in a healthy 78-year-old is often entirely expected and does not necessarily indicate disease, whereas the same value in a 35-year-old would warrant prompt investigation. Context matters enormously when interpreting eGFR results, which is why all three formulas supported by this GFR calculator incorporate age as a core variable.
| Age Group | Average eGFR (mL/min/1.73m²) | Clinical Interpretation |
|---|---|---|
| 20–29 | ~116 | Peak kidney function in most adults |
| 30–39 | ~107 | Normal, slight decline may begin |
| 40–49 | ~99 | Normal age-related decline |
| 50–59 | ~93 | Normal; annual monitoring if risk factors present |
| 60–69 | ~85 | Normal for age; eGFR 60–89 often not CKD in elderly |
| 70–79 | ~75 | Expected decline; interpret with urine albumin test |
| 80+ | ~65 | Age-related; CKD diagnosis requires other markers too |
It is important to note that an eGFR between 60 and 89 (Stage G2) alone is not automatically classified as CKD in older adults unless accompanied by additional evidence of kidney damage such as proteinuria, abnormal urine sediment, structural abnormalities on imaging, or a history of kidney disease. A single isolated eGFR reading is always less meaningful than a trend measured over multiple tests.
The Five Stages of Chronic Kidney Disease (CKD) by eGFR
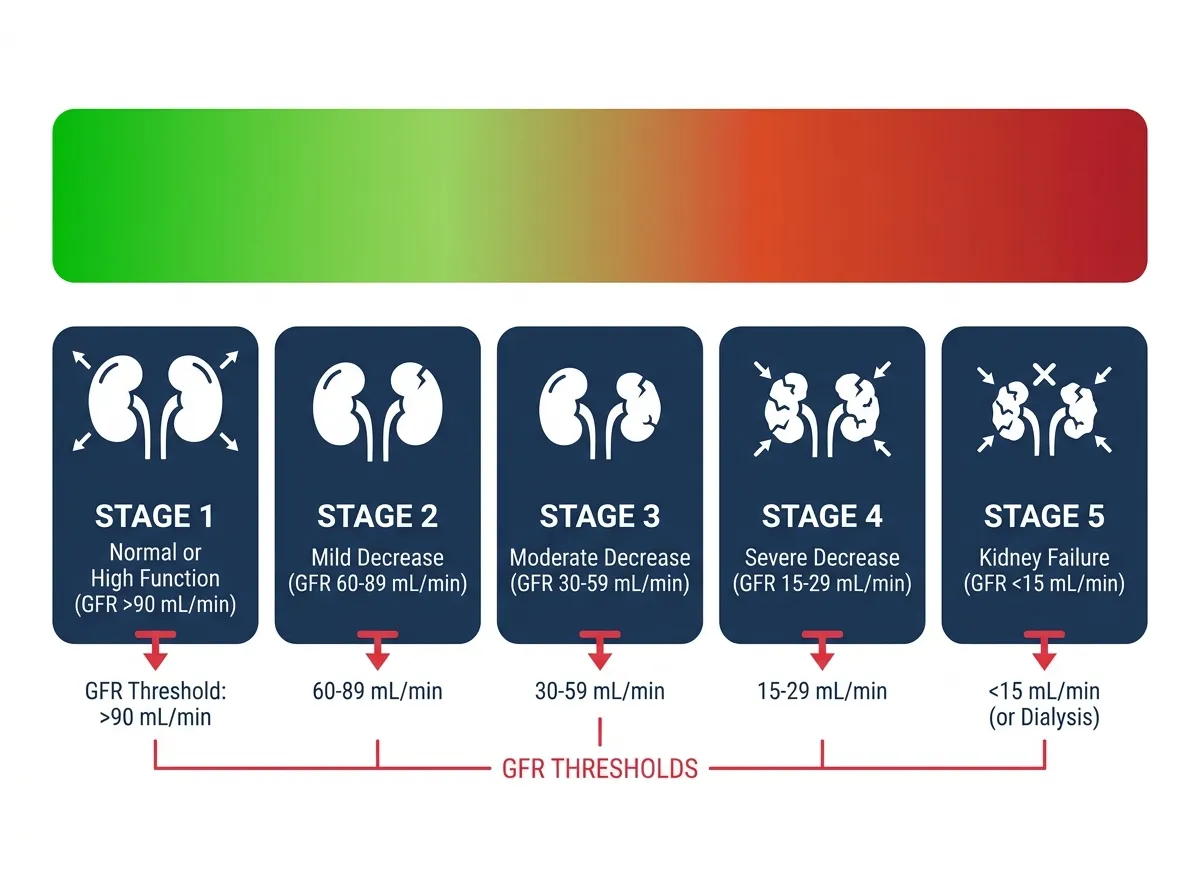
The KDIGO (Kidney Disease: Improving Global Outcomes) 2012 guidelines — still the international standard — classify CKD into five stages based primarily on eGFR, combined with the degree of albuminuria (protein in urine). Understanding your CKD stage helps determine the appropriate monitoring frequency, dietary modifications, medication adjustments, and when specialist nephrology care is needed.
Kidney function is normal or high. CKD at this stage is diagnosed only when kidney damage is present (e.g., proteinuria, structural abnormality). Focus on prevention and annual monitoring.
Mild reduction. Requires evidence of kidney damage for CKD diagnosis. Blood pressure control, diabetes management, and dietary modifications are the primary interventions.
Moderate decline in kidney function. Complications like anemia, bone disease, and fluid retention may begin. Nephrologist referral is recommended at Stage G3B or earlier if progressing rapidly.
Severe kidney disease. Active preparation for renal replacement therapy (dialysis or transplant) should begin. Nephrology care is essential. Medication dosing must be carefully managed.
End-stage renal disease. The kidneys have lost almost all functional capacity. Dialysis or kidney transplantation is required to sustain life. Contact a transplant centre immediately if not already under care.
Complete CKD staging also incorporates the albuminuria category alongside GFR. The urine albumin-to-creatinine ratio (uACR) — A1 (normal, <30 mg/g), A2 (moderately increased, 30–300 mg/g), and A3 (severely increased, >300 mg/g) — is a critically important companion test to eGFR. High proteinuria at any GFR level significantly accelerates kidney function decline and elevates cardiovascular risk. Diabetes and high blood pressure are the two leading causes of CKD in the United States, together responsible for nearly two-thirds of all cases.
CKD-EPI 2021, MDRD, and Cockcroft-Gault: Which GFR Formula Is Best?
This eGFR calculator supports all three major formulas used in clinical practice. Each has different strengths, limitations, and ideal use cases. Here is what you need to know about each GFR calculation method:
CKD-EPI Creatinine Equation (2021) — The Recommended Standard
The CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration) equation was updated in 2021 following a recommendation by the joint NKF-ASN Task Force to remove race as a variable. The 2021 CKD-EPI equation is now the recommended standard, and 2021 CKD-EPI creatinine is currently recommended by the ASN and NKF for GFR reporting in the United States. It uses serum creatinine, age, and biological sex, and is more accurate than the MDRD formula — particularly at eGFR values above 60 mL/min/1.73m².
× 0.9938Age × (1.012 if female)
κ = 0.7 (female) or 0.9 (male)
α = −0.241 (female) or −0.302 (male)
MDRD 4-Variable Formula — Legacy Reference Standard
The MDRD (Modification of Diet in Renal Disease) formula was the dominant clinical standard for many years before CKD-EPI was developed. It uses serum creatinine, age, and sex. While it tends to underestimate GFR in patients with normal or near-normal kidney function, it remains clinically relevant as a reference and is still used in some laboratories and studies. The MDRD formula calculates eGFR as: 175 × (Scr)−1.154 × (Age)−0.203 × 0.742 (if female).
Cockcroft-Gault Formula — Drug Dosing Applications
Developed in 1976 by Cockcroft and Gault, this formula estimates creatinine clearance (CrCl) rather than eGFR — a subtle but important distinction. Because it incorporates body weight as a proxy for muscle mass, it is the formula most used by pharmacists and physicians for adjusting medication doses in patients with reduced kidney function. The equation is: CrCl = ((140 − Age) × Weight in kg) / (72 × Scr), multiplied by 0.85 for females. It is less accurate than CKD-EPI for CKD diagnosis and staging, and should not be the primary tool for that purpose.
Just as the Heart Score Calculator uses validated cardiovascular risk models to estimate 10-year heart disease risk, this GFR calculator applies rigorously validated kidney function equations to give you a clinically meaningful result. For people managing both cardiovascular and kidney conditions — which frequently co-exist — tracking both numbers together is important. If you have not already, consider also checking your biological age score, as lifestyle factors such as physical activity, diet, and blood pressure management influence both kidney and cardiovascular aging simultaneously.
Serum Creatinine Levels, Muscle Mass, and Factors That Affect Your eGFR
Serum creatinine is the primary biomarker used in every standard GFR calculation. It is a natural waste product produced at a relatively constant rate from the breakdown of creatine phosphate in muscle tissue. Because healthy kidneys filter creatinine efficiently, elevated blood creatinine levels directly signal reduced kidney filtration capacity.
Normal serum creatinine values are approximately 0.6–1.2 mg/dL in adult males and 0.5–1.1 mg/dL in adult females (or 53–106 µmol/L and 44–97 µmol/L respectively), though laboratory-specific reference ranges vary slightly. Females generally have lower creatinine levels than males due to differences in muscle mass, which is one reason biological sex is a required input in all three GFR formulas.
Factors That Can Artificially Raise Creatinine (Lower Your eGFR)
- High-protein or high-meat diet in the 24–48 hours before blood draw
- Intense exercise or heavy physical activity shortly before testing
- Significant dehydration — reduces renal blood flow and filtration
- Certain medications including trimethoprim, cimetidine, and some NSAIDs
- Rhabdomyolysis (muscle breakdown from trauma, extreme exercise, or statins)
Factors That Can Artificially Lower Creatinine (Raise Your eGFR, Potentially Masking Disease)
- Low muscle mass — common in elderly patients, those with sarcopenia, or limb amputees
- Severe malnutrition or very low protein intake
- Advanced liver cirrhosis — reduces creatine production in the liver
- Prolonged bed rest or severe physical deconditioning
For patients in whom creatinine-based eGFR may be unreliable — particularly elderly individuals with very low muscle mass or people with liver disease — Cystatin C GFR provides a more accurate alternative. Cystatin C is a small protein produced at a constant rate by virtually all cells in the body, making it far less influenced by muscle mass than creatinine. The CKD-EPI 2021 Cystatin C equation and the combined creatinine-cystatin C equation are recommended by NIDDK when creatinine alone may give a misleading result. Cystatin C testing requires a separate blood test not included in standard metabolic panels.
High blood pressure (hypertension) and diabetes are the two most important conditions that accelerate kidney function decline. Both damage the delicate capillaries of the glomeruli over time, reducing filtration capacity. If you have either condition, regular eGFR testing — alongside blood pressure monitoring and blood glucose control — is essential. Proteinuria (protein in the urine) is another key warning sign: if you have a normal or near-normal eGFR but high urine albumin, your kidneys are already under strain, and preventive care should begin immediately.
How to Protect and Improve Your Kidney Function
While established CKD cannot be fully cured, its progression can be dramatically slowed through targeted medical management and lifestyle changes. For people in early stages (G1–G3A), consistent preventive care can preserve kidney function for decades. Here are the most evidence-supported strategies:
For people with Stage G4 or G5 CKD, proactive preparation for renal replacement therapy — including evaluation for kidney transplant listing, peritoneal dialysis training, or arteriovenous fistula creation for hemodialysis — should begin well in advance of ESRD. Early referral to a transplant centre offers significantly better outcomes than late referral. The Heart Score Calculator recommends consulting a nephrologist at any eGFR below 30, and considering early referral at eGFR below 45 if decline is rapid.