ABG Calculator:
Complete Arterial
Blood Gas Interpretation
The most comprehensive free ABG interpretation calculator available. Enter pH, PaCO₂, and HCO₃⁻ to instantly get primary disorder classification, compensation adequacy using Winter's formula, anion gap with albumin correction, P/F ratio, A-a gradient, base excess analysis, tic-tac-toe visual, and a full step-by-step breakdown. Built for nurses, respiratory therapists, medical students, and ICU clinicians.
Most ABG calculators just label the disorder. Ours gives you everything in one place: primary disorder, compensation status (with formula), anion gap + albumin correction + delta-delta, P/F ratio, A-a gradient, base excess, Henderson-Hasselbalch consistency check, tic-tac-toe visual, 6-step teaching breakdown, and a 5-case practice quiz — all free, no login.
⚠️ For educational use only. This tool supports learning and double-checking — it does not replace clinical judgment, senior review, or patient assessment. Always verify ABG interpretation in the context of the patient's full clinical picture.
ABG Interpreter
Clinical FormulasNormal: 7.35–7.45
Normal: 35–45 mmHg
Normal: 22–26 mEq/L · Calculated value
Normal: 80–100 mmHg
Room air = 21%
For A-a gradient
Normal: −2 to +2
Normal: 4.0 g/dL
ABG interpretation is a clinical skill — this tool assists with calculations and teaching, not clinical decision-making. Mixed disorders, artefactual samples, and patient-specific factors can all affect interpretation. Always correlate with the patient's history, examination, and trend.
Normal ABG Values: What Does a Normal Arterial Blood Gas Look Like?
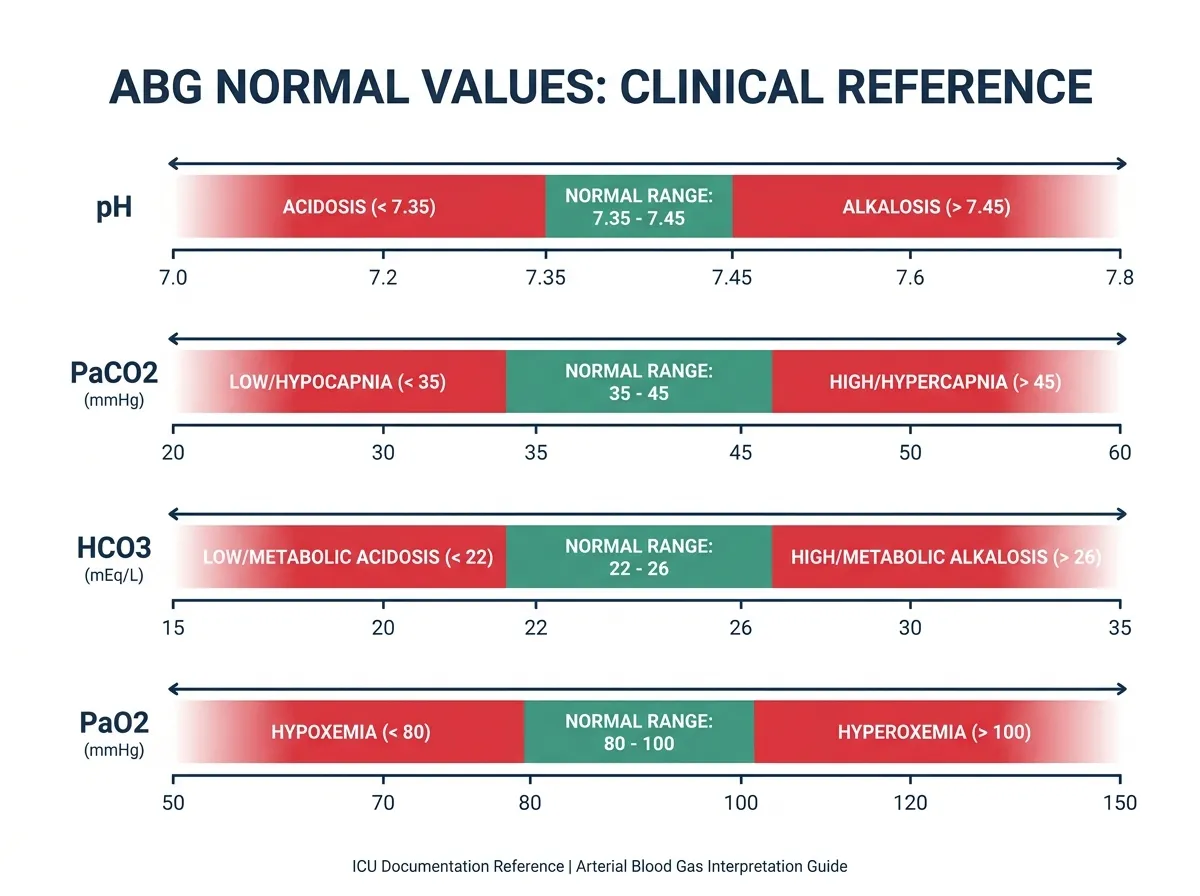
Understanding what a normal ABG looks like is the foundation of all interpretation. The body maintains these parameters within narrow ranges because even small deviations can signal significant pathology. What is a normal ABG value? The following reference ranges apply to healthy adults breathing room air at sea level.
| Parameter | US (mmHg / mEq/L) | SI (kPa / mmol/L) | What It Measures |
|---|---|---|---|
| pH | 7.35 – 7.45 | 7.35 – 7.45 | Overall acid-base status |
| PaCO₂ | 35 – 45 mmHg | 4.7 – 6.0 kPa | Respiratory component (CO₂ level) |
| HCO₃⁻ (calculated) | 22 – 26 mEq/L | 22 – 26 mmol/L | Metabolic component (renal buffer) |
| PaO₂ | 80 – 100 mmHg | 10.7 – 13.3 kPa | Oxygen level in arterial blood |
| SaO₂ | 94 – 100% | 94 – 100% | Haemoglobin oxygen saturation |
| Base Excess (BE) | −2 to +2 mEq/L | −2 to +2 mmol/L | Metabolic buffering capacity |
| Anion Gap | 8 – 12 mEq/L | 8 – 12 mmol/L | Unmeasured anions in plasma |
Which ABG values are measured vs calculated? Only three values are directly measured by the blood gas analyser: pH (via a glass electrode), PaCO₂ (Severinghaus CO₂ electrode), and PaO₂ (Clark polarographic electrode). Bicarbonate (HCO₃⁻), base excess, and standard bicarbonate are all calculated by the machine using the Henderson-Hasselbalch equation. This is why ABG interpretation guidelines recommend checking consistency — if the calculated pH from the Henderson-Hasselbalch equation differs by more than ±0.05 from the measured pH, a sampling or processing error is likely.
The Four Primary ABG Acid-Base Disorders
Every ABG abnormality falls into one of four primary categories, or a combination (mixed disorder). Understanding what causes each disorder is as important as recognising the pattern from the numbers.
| Disorder | pH | PaCO₂ | HCO₃⁻ | Primary Cause |
|---|---|---|---|---|
| Resp Acidosis | ↓ Low | ↑ High | ↑ (compensation) | Hypoventilation — CO₂ retention |
| Resp Alkalosis | ↑ High | ↓ Low | ↓ (compensation) | Hyperventilation — CO₂ loss |
| Met Acidosis | ↓ Low | ↓ (compensation) | ↓ Low | HCO₃⁻ loss or acid gain |
| Met Alkalosis | ↑ High | ↑ (compensation) | ↑ High | H⁺ loss or HCO₃⁻ gain |
Any condition that reduces alveolar ventilation, causing CO₂ to accumulate. Common causes: COPD exacerbation, severe asthma, opioid or sedative overdose, chest wall injury, neuromuscular disease (Guillain-Barré, myasthenia gravis), sleep apnoea, and inadequate mechanical ventilation settings.
Any stimulus to hyperventilation causing excessive CO₂ loss. Common causes: anxiety/panic attacks, pain, hypoxia-driven hyperventilation (PE, pneumonia, high altitude), fever, sepsis, hepatic encephalopathy, pregnancy (progesterone stimulates respiratory centre), and over-ventilation on a ventilator.
Either acid accumulation or bicarbonate loss. Use MUDPILES for high anion gap causes: Methanol, Uraemia, DKA, Propylene glycol/Paracetamol, Iron/Isoniazid, Lactic acidosis, Ethylene glycol, Salicylates. Non-anion gap causes include diarrhoea (HCO₃⁻ loss), renal tubular acidosis, and carbonic anhydrase inhibitors.
Most commonly hydrogen ion loss or bicarbonate gain. Causes: persistent vomiting or nasogastric suction (HCl loss), loop and thiazide diuretics (H⁺ + K⁺ loss), Conn syndrome (aldosteronism), Cushing's syndrome, post-hypercapnic alkalosis, excessive sodium bicarbonate administration, and milk-alkali syndrome.
ABG Compensation Formulas: How to Calculate ABG Compensation
Compensation is the body's attempt to normalise pH after a primary acid-base disturbance. The respiratory system compensates for metabolic disorders almost immediately (within minutes), while the kidneys compensate for respiratory disorders over hours to days. Understanding how to calculate ABG compensation tells you whether a second disorder is present — the key to identifying mixed disorders.
Winter's Formula — Metabolic Acidosis
Winter's formula is the most clinically important ABG compensation equation. It predicts the expected PaCO₂ after the respiratory system fully compensates for metabolic acidosis. If the measured PaCO₂ differs significantly from the predicted value, a second primary disorder is present.
Metabolic Alkalosis Compensation
Respiratory Disorder Compensation Rules
How to Calculate P/F Ratio from ABG
The P/F ratio (also called the Horowitz quotient) is one of the most clinically important calculated values derived from the ABG. It quantifies oxygenation efficiency and forms part of the Berlin Definition of ARDS. Learning how to calculate the P/F ratio from ABG is essential for ICU nurses and respiratory therapists.
How to Calculate A-a Gradient from ABG
How to Calculate Anion Gap from ABG
How to Interpret ABG Values: The 6-Step Method
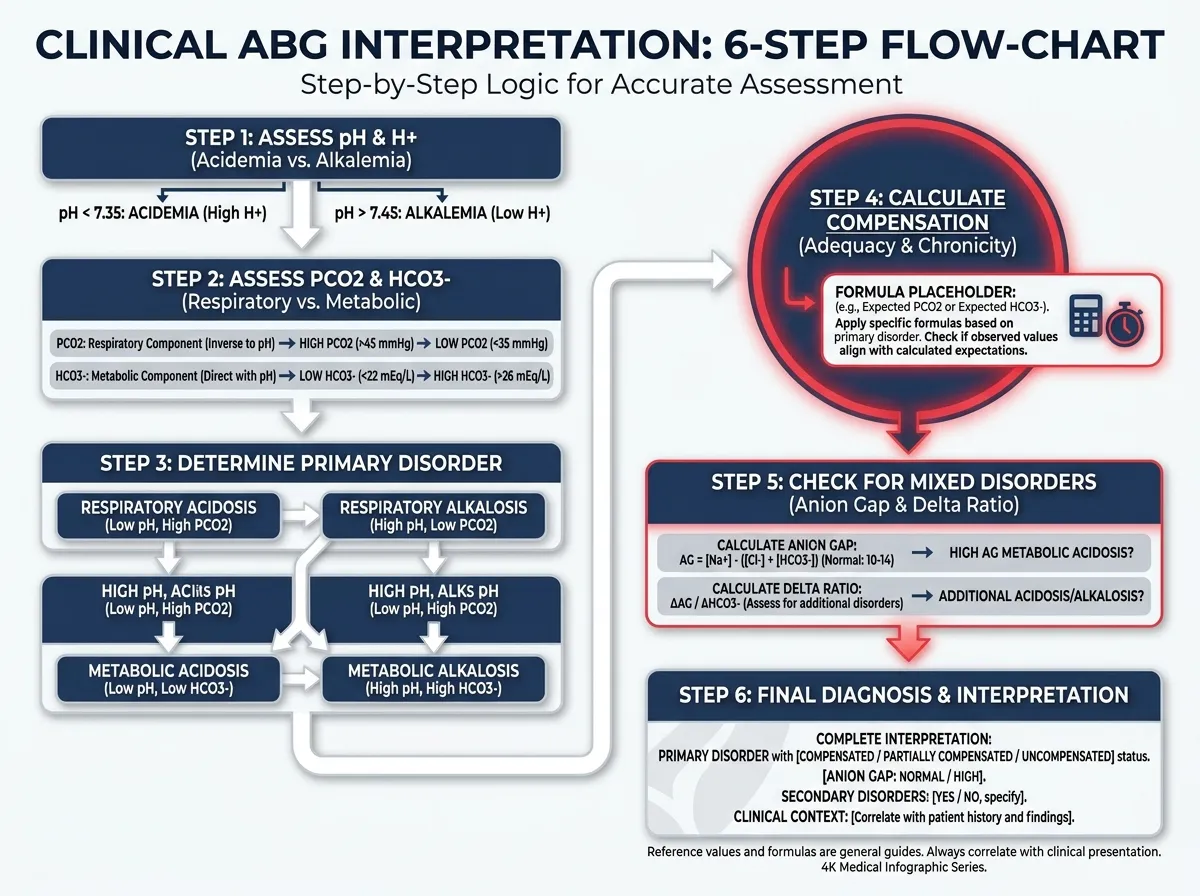
The most reliable way to interpret an ABG — whether you are a nursing student learning ABGs for the first time or an experienced clinician double-checking a bedside calculation — is a systematic six-step approach. Every step builds on the previous, and skipping a step is how mixed disorders get missed.
Evidence-Based Ways to Reach a Healthy BMI
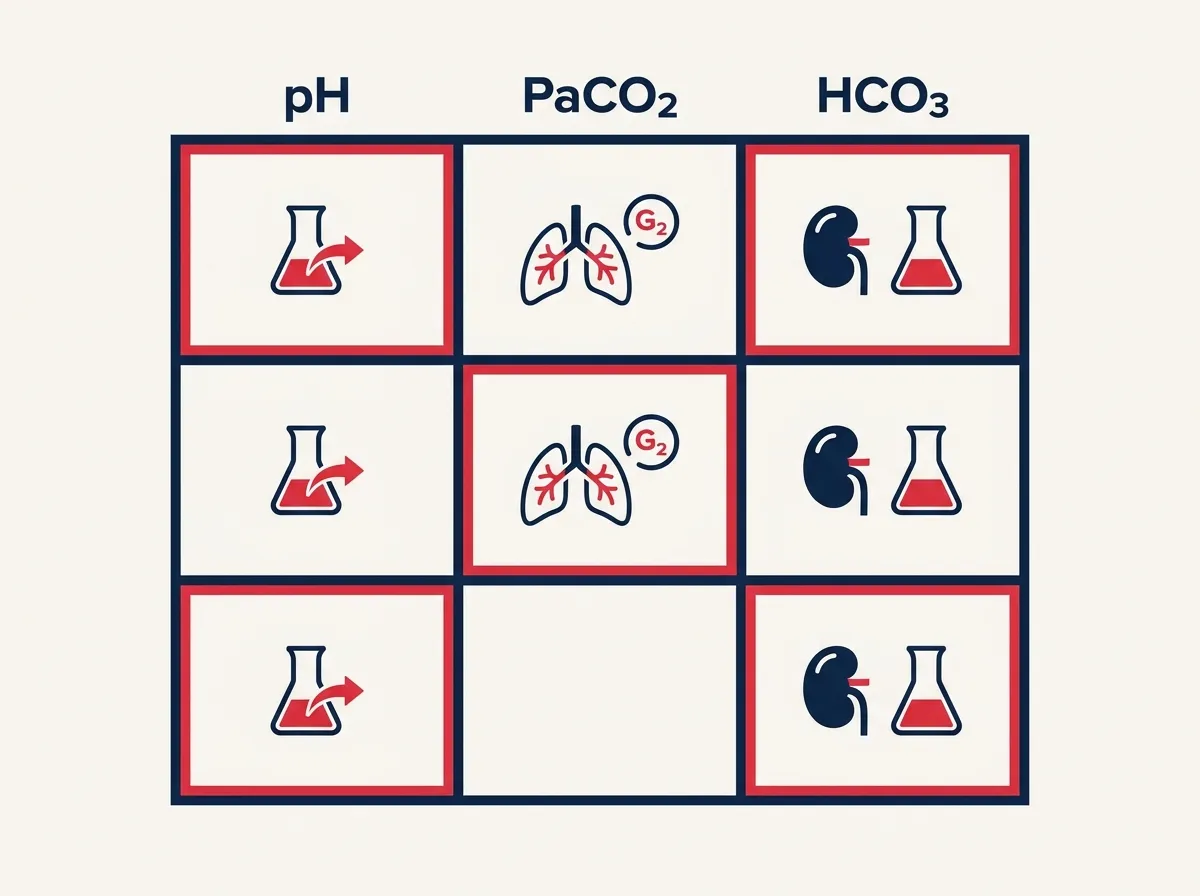
The tic-tac-toe ABG method (also called the ABG grid or 3-box method) is one of the most popular teaching tools in nursing education for quickly identifying primary acid-base disorders. It is especially useful for nursing students learning to calculate ABGs and interpret results at the bedside without needing to memorise complex algorithms. Our ABG calculator includes an interactive tic-tac-toe visual that highlights automatically after each calculation.
The tic-tac-toe grid places pH, PaCO₂, and HCO₃⁻ side by side with arrows indicating their direction relative to normal. The rule is simple: the two boxes that move in the same direction as each other identify the disorder and the compensation. When pH goes acidotic (↓), look to see whether PaCO₂ is high (↑) — if so, it is respiratory acidosis. If HCO₃⁻ is low (↓), it is metabolic acidosis. The third box showing a change represents compensation.
Quick Tic-Tac-Toe Rule: The two boxes that match the pH direction are your disorder. The third box that moves in the opposite direction to the disorder identifies compensation in progress. When all three boxes show abnormal values, always suspect a mixed disorder — this is where a compensation formula is essential to sort it out.
ABG Calculation Practice — 5 Clinical Case Quiz
The best way to master how to calculate ABGs is through regular practice with real clinical scenarios. These five cases cover the most commonly encountered acid-base patterns. Choose your answer, then read the full explanation — each case breaks down the ABG calculation step by step.